If you’ve ever read my posts on ER Safety, Hospital Safety, or the Hidden Corn- Medical Supplies post, you probably know that blood transfusions contain corn derivatives. I’ve known this a while and made plans for eventually having to have an emergency treatment that would require corn exposure in order to save my life. But I had always hoped it just wouldn’t happen to me. But of course it did, last July.
Slow Build
I’ve had blood tests showing mild anemia here and there for a lot of years. It was sporadic. Sometimes my red blood cell count would be fine but my hematocrit was slightly low. Sometimes rbc & hematocrit would be low. Other times my rbc and hematocrit would be fine, but my MCV would be high. My iron and b12 levels were always fine though, and my doctors and I always felt we had bigger problems to worry about, so not much was done to look into it.
I’ve also had many years of difficulty with what seemed like POTS symptoms (tachycardia when shifting position from laying down to sitting, or sitting to standing) that came and went seemingly with MCAS flares. Over the last couple years these episodes have been coming more and more often, but were still episodic. I kept chasing a POTS diagnosis but we could never manage to do testing while it was happening.
Crisis
Last July, I finally had a severe “dysautonomia” episode. Except it wasn’t.
What I experienced was a few days of feeling like I had “the flu” except my fever was never above 99°F. I slept constantly and felt too weak and tired to even write an email from my phone to let work know I would be out. After a day or two of this fatigue I began to have dark, tea colored urine which I perceived as “bloody” urine and thought I had a UTI.
After I was feeling less tired, I began to have tachycardia (rapid heart rate) whenever I changed position from laying down to sitting or sitting to standing up. This tachycardia would fade /normalize within a minute whereas in POTS it should continue for some time after changing position The tachycardia would also be accompanied by throbbing head pain that would pulse in time with my heart beat. This pain would happen if I even tilted my head without changing position. At times I would feel the throbbing pulsing in my lower back.
I also had some pretty bad cognitive deficiencies. I left a burner on and almost burned the house down, forgot names and common words, couldn’t remember things that had happened earlier in the same day. I also was so confused that I didn’t realize this was an emergency so I waited to see my regular doctor. I should have gone to the ER
My doctor did a complete blood count “just in case” and saw that I was pretty severely anemic. It turns out that the symptoms of an inability to regulate your own blood pressure and heart rate appropriately are really similar to the symptoms of just literally not having enough blood in your body. We had never done blood testing before during one of these episodes because I had so many other reasons to be dizzy and have irregular blood pressure.
She assumed I had some kind of internal bleeding, and called me back in to her office the following day to do some physical exams to see if she could determine the source of the bleed (she couldn’t) before sending me to the emergency room with my lab results and ER packet in hand. I knew I was likely to need inpatient care, so I also brought my hospital suitcase and made sure my freezer was stocked with frozen prepped food for someone to grab and bring in as needed. More details on my hospital prep in my Hospital Safety Post.

When we arrived at the ER, they triaged me in with 0 minutes wait time, and were actually pretty great about my MCAS instructions. They still managed to cause me a moderate reaction with a pre-filled saline flush for the IV, which it turns out contain preservatives even though the night nurse insisted it only had saline and nothing else. And the hospital itself was pretty bad for me airborne wise due to the cleaners they use, as it always is. I was wearing my Vogmask with the behind-the-head strap to create a tighter seal and make it more comfortable, but I wish I had had my respirator instead, so I have now put it in my hospital kit. You can see what respirator and masks I use on my product list page.
The ER concluded (as I had suspected) that I needed blood transfusions. Normally they would do these in the ER, but since I was a reaction risk, they admitted me before starting them. I was pretty darn scared because of how badly I react to the dextrose and citric acid when I ingest them, and these same derivatives are the ones used as anticoagulants in blood bags. To try to prevent a very serious reaction, we used a modified version of the TMS protocol for pre-medication when a reaction is likely:
- Solu-Medrol (Generic: methylprednisolone) 125 mg IV 2-3 hours before transfusions begin. Must be preservative free.
- Benadryl (Generic: diphenhydramine) 25-50 mg intravenously or intra-muscular 1 hour prior to surgery/procedure. Preferred brand for IV Hospira, NDC 0409-2290-03. Follow with 25-50mg every 6 hours as needed until transfusions/procedure is complete.
- Zantac (Generic: ranitidine) 150 mg or famotidine 20mg orally or intravenously 1 hour prior to surgery/procedure. Follow with same dose every 6 hours as needed.
- Administer 5-day steroid taper after transfusions are compelte. I did a compounded corn-free version of the medrol dose-pak.
We couldn’t find an IV h2 that was without preservatives so I took my own compounded. The iv benadryl was very important if possible because it’s far more effective than oral route. If you are worried about a reaction intramuscular benadryl will be almost as effective as intravenous but less likely to cause as severe a reaction as intravenous.
When we did the transfusions, I definitely reacted to them while receiving them, even with all the steroids going in my system. If we had somehow been able to hold off for several days it would have been better to start oral steroids 2 days ahead of the procedure, rather than a high dose right before, to give it time to build up.



I itched, flushed, and was tachy the entire time I was getting the transfusions, and also had bone pain and joint pain, but no asthma or rash and blood pressure was okay. They released me late into my second day at the hospital. The attending physician said I had hemolytic anemia, meaning I was making red blood cells just fine, but they were rupturing and dying early. He said he’d normally keep me an extra day for observation but that I was clearly constantly reacting to the hospital and he thought I would do better at home. He recommended a hematologist follow up ASAP and discharged me with care instructions to watch for reactions to the transfusions for up to 5 days after the procedure.
For the 5 days after, I would begin itching, flushing, and having tachycardia any time my round the clock benadryl, ranitidine, and steroids would wear off. By the beginning of day 5 I began to be able to tell that I would be okay off the steroids with just the benadryl, and by day 7 I was able to stop taking benadryl every 6 hours and just go with my daily meds.
Something else was going on, even while I was fighting all these reactions though: Other than the constant histamine-related inflammation, I was feeling freaking GREAT. All of the blood pressure problems, heart rate that fluctuated with body position/posture, and general feeling of weakness was GONE. I didn’t realize until that moment how weak and fatigued I’d been for years even during my “good” times. Even though my face was puffy and I felt someone had put itching powder in all my clothes, every time someone asked how I was doing, I would say, “AMAZING, now that I’m plump with donor blood!”
Unraveling the Mystery
Once I was a bit more stable, it was time to figure out what the heck happened to me. I went to a hematologist, and after running some tests to make sure I wasn’t still hemolysing, she formally diagnosed me with autoimmune hemolytic anemia. This sounded likely given that I had faced a lot of MCAS inflammation from traveling right before the episode, and had been running a fever during them time when I was feeling too sick to get out of bed. However I didn’t *like* the diagnosis because the treatment for it, as stated by her, was to basically try real hard not to get sick or end up in any state that would encourage my body to destroy blood, and if I did, to treat with steroids. If the hemolysis continued to be an issue, the next courses of treatment were a splenectomy, and possibly chemotherapy.
That didn’t make me feel too great already. Considering how much better I felt post-transfusion, I had probably been hemolysing frequently for years leading up to the crisis. I didn’t like the idea of just walking around wondering if I was going to destroy blood with no particular way to control it.
If that’s how it was, I was going to have to be okay with that and do what I could to calm my body down and stop it destroying blood. But I just had the feeling it was worthwhile to dig in to other possible causes of hemolytic anemia, especially if there might be a kind where I could have slightly more control than just hoping very hard. Someone from one of my MCAS support groups told me that she had learned about a condition called G6PD Deficiency, commonly called Favism, that causes hemolytic anemia when certain foods (legumes, *especially* Fava beans) and medications. This condition primarily affects people of asian, african, and mediterranean descent, although it can affect other populations as well.
Well, it so happens that I am southeast asian, and that I was eating Fava beans about 3-5 days before this crisis. I also was eating fava beans 1 year before when I had a similarly severe episode that we didn’t do any blood testing around. Before that, I had never eaten fava beans before in my life. It was just a delicacy at the farmers market and I took some home when doing my regular shopping there because they are delicious.
I requested my PCP to help me get tested for g6pd deficiency. It turns out testing isn’t always very accurate for women, especially right after a hemolytic crisis (more on this later), but we figured why not run it once and see what came up.
I was deficient. Just barely, because it was so soon after my hemolytic crisis, but still deficient, and false positives are not a thing with this test really.
We had a diagnosis. I did get a second opinion from a hematologist to confirm it, but she agreed, and so did my original hematologist that had diagnosed me with autoimmune hemolytic anemia, once she saw the charts.
More About G6PD Deficiency
G6PD Deficiency is a genetic deficiency of an enyzme caled glucose-6-phosphate-dehydrogenase, or G6PD. This deficiency causes all of my cells to be vulnerable to damage from oxidative stress. In particular red blood cells, since they are so simple and have no mitochondria, will literally be destroyed by this stress.
This blood destruction is actually triggered by a number of foods and meds, the most severe food being, of all things, fava beans. Which is why the common name for this condition is “favism.”
The list of foods and meds that you have to avoid are as deep as corn, and have a HUGE amount of overlap with corn. The question of whether it’s safe to drink tea or not when you have this deficiency is answered with discussion of how the tea leaves are processed, whether there are an artificial flavors added, and even the tea bags or packaging the tea comes in. When someone asks what is a safe toothpaste for g6pd deficiency (g6pdd for short), the answer is that glycerin, sorbitol, and xylitol are all to be avoided for g6pdd. Yeah, really. Does this sound familiar, corn allergy people???
I won’t go fully into what needs to be avoided for g6pdd, but I will give a rundown of the condition and risk groups, both for the sake of trivia and in case it helps someone else out. One thing that I’ve noticed as I’ve read into this is that a number of my weirder non-corn MCAS reactions are actually to items that are also G6PDD triggers. Apparently there are a number of antifungal/antimicrobial coatings used on things like pipes and faucets that are quite stable but would definitely cause oxidative stress for someone who is g6pd deficient. I think this may be the cause of my weirder reactions to water. G6PDD causes hemolysis, not allergy, however I feel my mast cells may have attuned to hemolysis triggers.
G6PD Deficiency is NOT rare.
It affects over 800 million people. There are some populations where 70% of people have it.
What 6PD Deficiency Is
- G6PD Deficiency is a mutation on the X chromosome that affects creation of the enzyme glucose 6 phosphate dehydrogenase, also known as G6PD.
- Red blood cells deficient in this enzyme become unstable and are destroyed in the presence of certain foods and medications.
- The worst of these foods are fava beans, soy, and most legumes.
- The worst non-foods are NSAIDs, tylenol, fluroquinolone antibiotics, anti-malarial drugs, sulfa drugs, and any petrochemically derived substance including most artificial dyes, flavors, and synthesized vitamins.
- The list of foods and meds that trigger this blood destruction are broad and deep. Basically anything that triggers “oxidation” is a problem. You know all those supplements and foods that have anti-oxidants? Well some foods, meds, and supplements have pro-oxidants.
- NOTE that anything that creates oxidative stress on red blood cells can destroy them when they are deficient in g6pd. So I am still at risk to lyse blood cells when I have an infection or a mast cell reaction.
Who It Affects
- The origins of this deficiency are from mediterranean, asian, south asian, african populations. But the deficiency is now found in all populations.
- Primarily diagnosed in men but NOT only present in men. Just harder to diagnose in women when they have it.
Three things I want to point out about inheritance of g6pdd deficiency:
- Contrary to what some outdated resources say, it is NOT a recessive gene. If you have it, it is expressed. This means that if you have two X chromsomes, and only one copy of the mutation, you are not a “carrier” of the deficiency, you have it.
- If you have even one copy of it you will be partially deficient. I am only partially deficient yet had this severe crisis and many issues over my life with anemia and the results of low level hemolysis that did not show up on tests.
- This deficiency is X chromosome linked. That means that if have one X chromosome and have g6pdd, any children you have who have two X chromosomes will be at least partially deficient. If you have two X chromosomes, and one of them has g6pdd, your children have a 50% chance of being deficient. If you have two X chromosomes, and your child with one X chromosome is deficient, *you are also deficient*. He could only have inherited it from you.
Health Effects
- In severe cases, hemolytic crisis, such as my recent hospitalization and blood transfusions.
- High ferritin- The inflammation from hemolysis can cause your body to hang on to ferritin. As inflammation decreases this should go down, but if you are low level hemolysing frequently you may see high ferritin stores somewhat often.
- G6PD causes a reduced glutathione deficiency, which is an antioxidant that has a lot of interplay with allergic and mast cell reactivity. I don’t really see from the g6pd support groups that there is a known connection between g6pd and allergy/mast cell disease, but I think it’s possible.
- Methylation defects/MTHFR: G6PD involved in the pentose phosphate pathway, one important pathway for making NADPH. NADPH is used in the MTHFR pathway. There is another pathway by which NADPH is created, so you will still have it, but less.
- Having reduced g6pd activity impairs your ability to deal with oxidative stress by reducing your amount of available glutathione. Glutathione is not directly part of the MTHFR pathway, but it comes up a lot in discussion of related mutations. This is essentially restating the entire definition of g6pdd, however I felt it was important to frame it as part of the methylation stuff for people who are looking into that for themselves.
- Low-level hemolysis can have all kinds of long term health effects that basically look like chronic illness and an inability to detox. This is due to an overtaxed system due to both the high level of creation of new blood cells and the low tolerance for oxidative stress.
Testing & Diagnosis
The definitive diagnosis is a molecular test that checks the total quantity of g6pd in your blood sample. There are a couple of problems with this:
- This deficiency is only carried on the X Chromosome. If you have two X chromosomes, you likely only have 1 X chromosome with the defect, so the other X chromosome will correct for that and only some of your blood cells will be defective. This means your total g6pd count will be closer to normal, especially if you recently destroyed your more g6pd deficient cells.
- If you just finished with a hemolytic event, you can have a false normal because you lysed all the older, deficient blood cells. In men, this is true because the younger blood cells will have less of an overall deficiency than the older ones. In women, this is true for the same reason AND because of point #1.
It so happens that my quantitative test was deficient/positive for g6pd deficiency. This surprises me because of point 1. It makes me wonder if I either have two deficient x chromosomes, or a large number of my cells underwent lyonization.
If you wanted to get tested, I would start with the quantitative test. It’s very easy and labcorp does it. Quest probably does too.
HOWEVER if your test is negative, it doesn’t necessarily mean you don’t have it because of what I wrote above. If you are eating lots of beans, using NSAIDs, or even taking benadryl daily (yes benadryl can cause some blood destruction for g6pd), you may be destroying all your deficient cells. In this case, the way to make sure would be to avoid g6pd triggers for a few months and test again, or look for genetic testing, which is expensive and difficult.
23 and me won’t cut it. They only test a couple dozen of the SNP’s and there are literally hundreds of kinds of g6pd. I didn’t have any of the major SNP’s on 23 and me and only one of the minor ones. None of the interpreter services considered my results indicative of even a chance of g6pdd deficiency yet I am deficient. Mayo has a genetic test for it available, but I don’t know how much it costs.
Further Information
There’s a lot of conflicting information out there about what is and isn’t okay for g6pd deficiency, especially when it comes to diet. The best avoid list, in my opinion, is the most conservative one, because even low-level hemolysis is something that’s best to avoid. This avoid list on g6pdhelp.com is a good one. For generalized information, the G6PD Deficiency Foundation seems to have a fair amount of good resources and articles.
What This Means For Me
Well, my ER packet is 3x longer than it used to be and has a table of contents now, so that’s fun. I made sure to keep the hematologist who diagnosed me with the condition on my physician consult list because if I end up in an emergent or surgical type situation we’re really going to need her. I’ve already run into some complexities trying to get medical care for other conditions- I have arthritis symptoms as part of my MCAS reactions and my rheumatologist wanted to prescribe Plaquenil which is a big nono for G6PDD. That sucks because it sounded like it could help out a lot. I’m also seeing some concerningly blase attitudes about the condition from doctors, and am not sure how seriously they’ll take it in a more urgent situation like a hospital setting. That worries me some.
If I didn’t already have the corn allergy, the dietary and lifestyle changes would be a much bigger deal. All vitamin fortification is an issue for g6pdd. Cross contamination with soy like pre-seasoned cast iron pans using soybean oil as a seasoning , or ingredients that are commonly soy derivatives such as glycerin, xylitol, etc, or any and all added vitamins are problems for g6pdd and are overwhelming for newbies. On the other hand, I was already avoiding these things because they are also frequently corny.
I’m not able to eat the corn free legumes I had anymore, but that’s fine tbh. It’s a little bit of a pivot and I’m worried about having a lack of protein source variety. If I have too few options and have an interruption in food supply I could end up going hungry. I ran out of beef for a month once and lost like 15 lbs that I didn’t actually have to lose. But the amount of fatigue I had when I was eating them was so bad that it feels well worth it.
I’m really glad overall to have a certain amount of control over whether I destroy blood again. However it’s not 100% control. If I get sick or have a big reaction, or if I have an airborne exposure to chemicals (or fava bean pollen, apparently!) I could still hemolyse, and there would be no preventing that. But I can do a lot to maintain my health and lessen the chance of hemolysis.
Learn something from this post? Feel free to show your appreciation with a tip! The info on my blog is always free, so you are never obligated. But it is always appreciated.
![]()

Wow. What an experience. I am still digesting all the details, but I just wanted to check in and say thanks for sharing, as always, and I am so glad you made it through!
Have you seen the mast cell work at Tufts?
http://sackler.tufts.edu/Faculty-and-Research/Faculty-Research-Pages/Theoharis-Theoharides
Heard a podcast where he discussed some useful details and thought of you,
Episode #58: Mast Cell Master with Dr. T.C. Theoharides, PhD, MD from BetterHealthGuy Blogcasts
I am a female who Drs termed as the carrier of G6pd. I have been borderline anemic my whole life, seems to have a hemoglobin drop when I get sick, or just lethargic from eating certain foods or take certain medications.
My hemotologist try to brush it off as females doesn’t have any issues when they are the carriers. I have heard otherwise and was told to do a lyonization testing. I may have an inactive X Chromosome .
I am so happy to read your post. I don’t feel crazy anymore.
Hi Ann! I’m glad you found this post. Your doctors are incorrect. G6pdd is not a recessive gene, therefore you are not a carrier, you are partially deficient. Which as you noted can manifest as full deficiency due to lyonization. Here is more info on that, and please also use the rest of this site as a reference for how to avoid hemolysis triggers. I think you will find that by treating your g6pdd with diet and medication avoidance, you will not only stop your anemia but have a number of health improvements you couldn’t have predicted.
http://g6pddeficiency.org/wp/g6pd-deficiency-home/women-with-g6pd-deficiency/#.WpwecqCIY0M
Hi,
I have been doing a lot of reading on G6PD deficiency and I found there is a link to angioedema in G6PD deficiency due to bradykinin release during an episode; Your MCAS could be another expression of G6PD deficiency.
Thank you for the info! I am strongly convinced they are connected/interrelated and that my MCAS is as bad as it is because of the g6pdd. There is family history on the side that the g6pdd does NOT come from of EDS and mast cell, so it’s not the whole story, but it’s absolutely a large piece of the puzzle.
hello there 🙂 thanks for the article. I have G6PD and I really need an advice for which foods I need to avoid. I know I should avoid some nuts and foods and more importantly Fava beans but the problems is, it seems there is a vast kind of foods, fruits and nuts which we should avoid. so question is: technically every food will make us weaker? cause there is at least small amount of triggers is typical meals. can we avoid all those things with a plan? or just avoiding fava beans and some drugs is enough and we can’t avoid other thing and should remain kinda weak always? thanks and sorry for big question 😀
Hi there,
This site will answer most of your questions.
http://g6pddeficiency.org/wp/
No, it’s not enough to just avoid fava beans and a few meds. We need to avoid EVERYTHING on the list. But the list is not as long as you seem to think and does not include nuts or fruit.
Essentially we need to avoid sulfites, menthol, artificial blue coloring, artifical vitamin C, vitamin K, quinine, tea extracts, some chinese herbs, and all legumes.
http://g6pddeficiency.org/wp/living-with-g6pd-deficiency/g6pd-deficiency-foods-to-avoid-list/
The list of legumes is quite long and does contain peanuts which are a bean not a nut.
http://g6pddeficiency.org/wp/living-with-g6pd-deficiency/food-to-avoid/
But fruit is not on that list anywhere.
It is very easy to eat a varied diet rich in fruits, vegetables, seeds, and nuts and completely avoid all g6pdd triggers. There is a recipe section on that site to give you ideas.
Oh nice. thanks for the reply 🙂 btw i read somewhere there are 400 different mutation of this allergy. and other foods might trigger this … blood test can exactly identify each of these 400?
There are at least 400 genetic variants, but only 300 of them have been identified. A genetic test may be able to identify which variant you have, but if you don’t show up with one of the known variants on a genetic test it doesn’t mean you don’t have it. It just means you don’t have one they know how to test for. Also genetic testing is very expensive and insurance typically does not cover it.
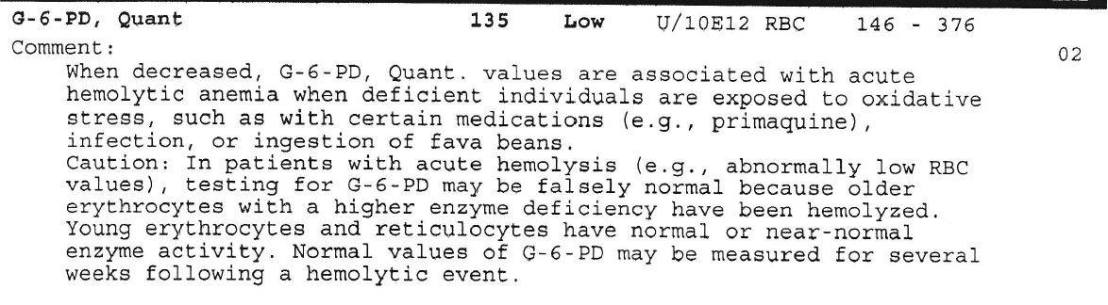
The definitive test for g6pdd is by counting how much of the actual g6pd enzyme you have. That is called “quantitative test.” That is what the blood test result I posted above is from. This test is not infallable- as the test result shows, if you have recently destroyed a bunch of blood, or if you are female who is only partially deficient, you may have a false negative. But if you have not hemolysed recently and are not eating trigger foods, it is an accurate test.
My recommendation for those that suspect g6pdd is:
1) Get the quantitative tests. If it is positive, you know you are deficient.
2) If it is negative, but you are eating legumes and other trigger foods in your diet or have taken medication or had an illness that may have caused you to hemolyse, wait a few months and avoid all g6pdd triggers, then test again.
Oh great explanation thanks ^_^
I’m sure i have G6PD. when i was a child apparently they even changed my blood and I have a lab certificate that i have G6PD. now when I eat fava beans sometimes I get really weak. but its delicious :)) so, is it important for me to know which kind I have among those 300?
It’s not important at all for you to know which variant of g6pdd you have. It IS however important for you to stop eating all legumes and especially fava beans.
If you are not allergic to corn, you should be referring to this site instead: http://g6pddeficiency.org/
My baby was just diagnosed with this… Never heard of this before
Me neither, until I was diagnosed with it. I would definitely read everything on g6pddeficiency.org. The author of the site has a Facebook support group as well.
ya I’m already on both lol
😉
It’s frustrating for me though because the doctors are still trying to give my son formula although there is no safe formula for a G6PD baby 😦
Yeah, and additionally there is really no corn free formula either. So in general, either way, no formula. Dale Baker or someone from the Facebook group should have some academic papers showing why ascorbic acid and soy are contraindicated for g6pdd. If you want to discuss corn derivatives with them I do have a few papers that discuss corn allergy reactions to corn derivatives linked throughout this site, but I am not sure if you want to fight both that battle and g6pdd with disbelieving doctors.
Question about g6pd deficiency. My mom has recently been diagnosed with autoimmune hemolytic anemia and put on corticosteroid therapy, which isn’t working. Her hgb and hct stay low. I know she has MTHFR deficiency. Could g6pd deficiency be the reason why she’s resistant to the corticosteroids working? Once you started avoiding all the g6pd triggers did your hemolytic anemia resolve? She just broke her hip and had to be transfused, how long should we wait to test her for the g6pd?
I’m sorry, morning brain. I meant MTHFR mutations, not deficiency.
Hey, Ellen, I have no idea if you’ll see this but I just read your question again and didn’t understand initially. Steroid therapy not working to stop autoimmune hemolytic anemia could be because the hemolysis isn’t autoimmune. That wouldn’t be steroid resistance, it would be. The steroids not working because the problem isn’t her immune system.
Your mom could look into g6pd deficiency. There are other non autoimmune causes of hemolysis out there probably as well. If she wanted to test do g6pdd she would want to do a genetic test though because if she’s lysing blood currently or has been recently she might get a false negative. If she has it, you could as well.
Hi, no, g6pd deficiency would not cause resistance to steroids that I’m aware of. The only medication interactions I’m aware of having to do with g6pdd are when the meds are a trigger that causes hemolysis, aka blood explosion.
Wow this is intensely fascinating. As a medical student it further informs me of how to work with and kindly treat with delicacy and understanding this situation in patients and not just brush them off as “difficult”. It will help to better understand the importance of compounded medicines free of additives and dyes. It’s also important for me to know this personally. I was diagnosed with G6PD in 2017 and I was dumbfounded. I was also anemic and the NP was scratching her head wondering why I was so chronically anemic. On top of being diagnosed with MCAS. I am taking much better care of myself now. Please keep this information coming. Hoping for your recovery, healing and strength. Sending much love and blessings to you.
Glad it’s been helpful. It’s been a wild ride learning how to live with the g6pdd. You’re probably in a better position than me to understand it but since this incident I’ve been leaning that this metabolic disorder does more than just cause hemolytic anemia. It’s also how we process sugar so we’re at risk for diabetes as well. Other stuff I’m still not totally clear on.
If you haven’t been going by Dale Baker’s avoid list for your g6pdd, please consider doing so. He’s got a number of references on his site backing up his claims. My feeling is that it’s pretty hard on our bone marrow to be making extra blood all the time, and given that we’ve already got misbehaving blood cells (MCAS), following the most conservative avoid list can only help. As with the corn allergy (and MCAS) when it comes to medical treatment we often have to choose the best from bad options, so I also feel that living my daily life avoiding the longest list of triggers possible puts me in a better position to handle medical treatments that may be less good for my blood.
Glad you are finding some answers. I seem to have not enough of an enzyme, diamine oxidase (DAO), that helps to digest histamines in foods and so have to avoid high histamine foods. (This is self diagnosed.) Wonder if that is related to what you are writing about? I experienced anaphylactic shock reaction from taking Benadryl, and a strong but not anaphylactic reaction to Tylenol. I have hives, etc. from nearly all meds. I also have a strong corn allergy (as well as from some other foods). Right now I am trying to determine if I can have the Covid vaccine because I have read that two of the components are corn derived: polysorbate 80 and polyethylene glycol. I will be seeing my physician for an annual physical soon and will see what she can help me with or get a referral. Also, this might be of interest to you and others. My health got much, much better after I started eating only whole food plant foods with no added oil, sugars or salt. Really love my vegetables so it is great. Have noticed that legumes are not great for me and can eat only rice or sometimes oats for grain in my diet. There is a lot of information just now on plant-based healthy recipes.
Wow sorry I somehow missed this for like four months! So I do know what DAO is and am aware of histamine intolerance and low histamine diets. Just to confirm that those are valid and real things and that your self diagnosis is valid. If you can’t eat high histamine foods and notice DAO supplements help you, that’s probably real. 🙂
Keeping in mind that I’m not actually very good at microbiology or genetics: I don’t think it’s related other than it having to do with the complex chain of metabolism that goes on in your cells as they do all the things they do. The pathways g6pd is involved in don’t really have any overlap with the ones DAO are involved in… but the precursors and products of each do eventually make them relate to each other. But not like, in any direct way.
Sterling’s explainer on how all these tie back to MTHFR may at least help frame the relationship in a high level way. Which is all I’m capable of lol. https://mthfrsupport.com/2016/03/when-other-genes-are-not-functioning-they-can-impact-mthfr/
My guess as far as legumes not being great for you that it could be a general sensitivity to oxidative stress that isn’t clinically g6pd deficiency, or simply that the lectins in them aren’t great for you. A lot of people have intolerance or mast cell issues with legumes for reasons that don’t have to do with g6pd enzyme. If you were worried about it though, you could always get your serum g6pd levels tested.
Anyway what I’ve found with both my other methylation related genetic polymorphisms, as well as the g6pd deficiency, is that while they create a predisposition to not processing or using things well, the severity of how they manifest can be influenced by other systems of the body. For example, any and everyone has reduced amounts of g6pd enzyme when they are hypothyroid, and it so happens that my g6pd deficiency became severe and life threatening when my hashimoto’s flared and my thyroid dumped. Getting my thyroid taken care of a little better has helped me be less likely to just destroy blood from every little exposure to g6pd triggers. I still control my diet carefully, but i was finding myself anemic if I got exposed to fog machine fog made from petroleum or fumes from isopropyl alcohol. That seems to have calmed down at least.
Similarly, something like 30% of people have one or more of the SNPs associated with MTHFR, DAO, COMT, CBS, and related. Not all of them are sick/histamine intolerant. So there is likely something else going on that is making us more susceptible to these variations of metabolic function. It’s not a sure thing, but I suspect if we can work on our root cause (which won’t be the same for all of us) there is a hope for having to be slightly less limited and careful. Best wishes on figuring out your root cause!