
What is Hypermobility?
Hypermobility refers to unstable joints that bend farther than they should. Many hypermobile people do not realize that what they do is out of the range of normal motion or that it could harm them, until they start having pain. And then often when hypermobile people finally DO have pain, it gets misdiagnosed as something else because what hypermobility is and what it can cause is so poorly understood.
Not only did I spend most of my life not realizing that my chronic pain was caused by my hypermobility, I was so convinced by others in my life that my pain was “normal” that it took me a long time to even admit that I was different.
When someone first told me I was hypermobile and should look into EDS, I told them that I didn’t have chronic pain. Except for the part where I had some amount of pain every single day, and people without chronic conditions go days or even weeks of their lives without feeling pain unless they are injured. I didn’t feel that I had any physical abnormalities or “loose” joints even though I injured my rotator cuff parallel parking my car at age 18, and had fully dislocated my hip around the same age doing kicks in a martial arts class. I thought I couldn’t be hypermobile because I couldn’t do splits, but I had all kinds of party tricks I could do with my bendy hands and fingers, and historically *used to* be able to do a number of flexibility tricks that I stopped being able to do because of what turned out to be osteoarthritis.
Everything I described in the previous paragraph is a symptom of my hypermobility, and is not typical. I wish I had understood that a long time before now. It would have saved me a lot of pain and rehabilitation time.
Here’s what I wish patients, practitioners, family, and friends understood about hypermobility.
Things I Wish Everyone Knew About Hypermobility
- Hypermobility is NOT rare.
- It’s not just human pretzels – Hypermobility is not the same as being flexible.
- Hypermobility can affect more than your joints.
- Hypermobility is linked with mast cell activation disorders.
- Hypermobility pain is treatable.
- Even if you “only” have hypermobility and not Ehlers Danlos syndrome, you still need medical care for your symptoms.
Hypermobility is NOT rare.
At least 3% of people have Joint Hypermobility Syndrome. That’s about 9 million people in the United States. This is a conservative figure: other statistics place it closer to 20% of people.
It’s Not Just Human Pretzels: Hypermobility is Not the Same as Being Flexible
Many people confuse being hypermobile with being “flexible”, and think if they aren’t contortionists or can’t do splits that they can’t possibly be hypermobile. This isn’t true.
Flexibility refers to your muscles being able to lengthen. Hypermobility refers to your ligaments lengthening. This lengthening may not cause inflammation and pain in the tendons and ligaments when someone is young – but it may begin to happen with age. Regardless of whether the ligaments or tendons become painful or damaged, their laxity creates a situation where your joints just don’t stay fully in the socket and slide around in the joint space and damage the cartilage, and this can cause bursitis and/or osteoarthritis. Again, it is common for joints to “feel fine” when younger and become damaged with age.
Depending on the person and the type and degree of hypermobility, these hyperextensions causing pain “with age” can mean age 10, age 20, age 30, or even age 50+.
Hypermobility Can Cause the OPPOSITE of Flexibility
Because your ligaments are not holding your joints together, your muscles may overcompensate. This will actually lead to stiffness and lack of flexibility. When you are hypermobile, trying to stretch a stiff, spasmed muscle can pull or irritate ligaments or tendons, either subluxing a joint or causing tendinitis.
Note: This doesn’t mean don’t stretch, and it doesn’t mean don’t exercise. It just means that the typical methods don’t apply.
“Double-jointed” Isn’t Actually a Thing
Many people who are hypermobile say they are “double-jointed,” which is seen as a benign condition. There is no such thing as being “double-jointed.” There are no special joints that are different, doubled, or in some other way “designed” to bend too far. There are just joints whose ligaments stretch rather than holding the joint in place, until they do eventually sustain damage from the instability – which causes pain.
Many health resources say that hypermobility is not a problem unless it causes pain. I disagree – I say it’s only a matter of time until it DOES cause pain.
Hypermobility Can Seem Subtle (if you don’t know what you’re looking for.)
I’ve already told you that hypermobility doesn’t necessarily mean you’re a contortionist or that you can do splits.
The “Beighton Score” is meant to determine joint hypermobility, and certainly if you can do any one of those tricks, you have at least one hypermobile joint and should probably STOP doing that trick to avoid future joint damage.
But more pragmatically, these are the things I notice in hypermobile people that leads me to suggest that they have their beighton score evaluated, and also include any things they could historically do but can’t any more:
- If you can scratch/wash every part of your back. (This is not considered within the typical range of motion.)
- If you can zip up your own back-zip shirt or dress all the way up, even when the back goes up high. (See above.)
- If you sometimes feel like one or more of your joints is just “a little bit” out of place, but have dismissed that as not possible. (Actually that could be literally what is happening. This is called a subluxation.)
- If you have sustained a sports injury (rotator cuff tear, tendinitis found primarily in athletes, full joint dislocation) from doing a normal, daily, non-sporting task. (If your ligaments are lax, or the joint is unstable, “normal” activities may strain your body as if you were engaging in athletics.)
- If you have one or more “party tricks” you can do like putting your feet up over your head or bending your fingers backwards or at crazy angles. (There is no such thing as double-jointed, remember? You are hyperextending or subluxating something.)
- If you USED TO be able to do those “party tricks” but you can’t anymore because it hurts now. (The joints are now damaged due to the hyperextension/subluxation.)
- If your hands, elbows, knees, or shoulders just always look “weird” in pictures like they’re at the wrong angle and you don’t know why. (Probably they look weird because you’re hyperextending.)
- If you can balance your smartphone on one finger and use your thumb to reach EVERY part of the screen without moving your hand at all. (No, this actually isn’t a normal range of motion unless your phone is very small or your hand is VERY large.)
- If when you lock your knees and look at them in the mirror, your kneecaps flatten out and you see “dimples” over them. (That “dimple” indicates hyperextension.)
- If you are an adult and can “W” sit, or you could into younger adulthood but stopped being able to as an older adult. (This indicates an abnormal range of motion in your hips and/or knees and is something only children “should be ” able to do.)
- If you have super soft skin and/or look young for your age. (Hypermobile collagen often doesn’t wrinkle as easily.)
It’s Not Just Your Joints
If you have HSD and not EDS (more on that below), it’s *mostly* about your joints, but there are other effects to hypermobility such as:
- Small fiber neuropathy
- Disturbed/atypical proprioception, often classified as “clumsiness”
- Flat feet (because the connective tissue holding your arch shape is soft)
- Skeletal changes due to soft connective tissue: kyphosis, scoliosis, lordosis, or misaligned bones in the feet and arms.
- Digestive issues/IBS
- Dysautonomia/orthostatic tachycardia
- Pelvic and bladder dysfunction
- Obstructive sleep apnea
- Poor blood circulation and pooling of blood in the extremities, often leading to dizziness and fatigue
- Weak, fragile, or “stretchy” veins which burst easily and/or are hard to draw from
Hypermobility with or without the above is known as Hypermobility Spectrum Disorder. Hypermobility with “other stuff” affecting the internal organs and veins (see below) is probably Ehlers Danlos Syndrome, unless there is some other medical explanation for the symptoms.
Hypermobility is Linked with Mast Cell Activation Disorders.
Hypermobility and MCAD’s are linked not just epidemiologically, but the connection is thought to be causal. More about this connection form Anne Maitland in this youtube video. I have a blog post with more info about mast cell disorders in general.
In my case, my MCAD/MCAS reactivity is *so* tightly coupled with my hypermobility that I will actually have joint subluxations and pain as a direct result of a mast cell trigger exposure. Once I realized (from an older Maitland talk) that these could be connected, I began to notice that I would have a really good week, then get a face full of perfume or fabric softener, and within five minutes experience a hip subluxation for which I required crutches or a wheelchair.
Once I got on a daily med, ketotifen, that helped me with reducing the severity of my airborne reactions, I attended a sci fi & fantasy convention that I would normally have needed a mask to attend. I was amazed to realize that I could totally handle *most* of the con without a mask, so I didn’t wear one. By day two of the convention, I was having so much trouble with my knees and hips that I needed crutches. By day three, my wrists were so bad from the crutches that I needed a wheelchair. I didn’t put together that I was having delayed/systemic reactions to the cleaners and scents from the hotel and convention guests until someone else suggested that. I tried upping my rescue meds and almost *instantly* had a reduction in pain.
So while I employ a BUNCH of methods for treating my EDS pain, detailed below, my personal first line of treatment is actually to treat my mast cell reactivity!
Hypermobility Pain is Treatable
There is no cure for hypermobility, but many people can actually get a LOT of function back and reduce their pain quite a bit with the RIGHT kind of treatment.
Treatment centers around both adjusting your ways of doing things to avoid injury and strengthening your muscles to increase joint stability and reduce daily damage and wear. This sounds basic and like it can’t possibly help much, but I can personally attest that I went from *extremely* low function and high pain to going weeks at a time without any basic daily life activities being impacted by my pain or dislocations. And the PT that I did to get from hardly being able to take care of myself at home to actually getting out and doing life felt like things that could not POSSIBLY be helpful. It was just so slow and gradual, which it has to be for EDS.
It is absolutely CRUCIAL though that any physical or occupational therapy be done right and guided by knowledgeable practitioners, because it is so easy to injure a hypermobile person with the wrong kind of exercise, the wrong order of strengthening, or going too fast and adding too much resistance before muscles are ready, forcing the tendons and ligaments to take up the slack.
Finding the right providers can be very difficult, unfortunately. More and more people are learning about it, but there are still far more people that don’t understand hypermobility than do. Your best bet is to reach out to local patient communities to find out who is helping other people with hypermobility and/or EDS.
Another option is to do some self-study and ask a PT who’s less familiar but willing to listen to work with you to learn how to help and treat you without harming you. For self study resources, see below.
Hand Therapy Exists
This is about treatment but it gets its own headline because I really, really wish I had known this before I did. Hand therapists are often occupational therapists, and sometimes physical therapists, who specialize in treating and rehabilitating your hands.
Since your hands have very little muscle mass compared to the rest of your body, and since you use them for nearly all daily tasks, hands can be the part of the body that start malfunctioning first on a hypermobile person, and are among the most disruptive to basic tasks when they do.
Much like many other aspects of hypermobility pain, many people with hand pain do NOT realize that hypermobility is the cause of their pain. I sure didn’t. If I had gone to a hand therapist, they probably would have realized that was the case sooner than I did. Not sure though, given that physical therapists that don’t specialize in hands and aren’t familiar with hypermobility don’t always realize that’s the issue or how to treat it. BUT once I did know it was hypermobility, I wasted a lot of time self-treating and paying cash for items like splints that a hand therapist could have helped me with *and* gotten covered by insurance.
So, this is me letting you know that hand therapy is a discipline at all. Finding a hand therapist that understands EDS/hypermobility is important, but my personal experience is that more of them know what it is than PT’s I talk to.
CORN ALLERGY WARNING: Some hand therapists do Fluidotherapy, which involves literal corn husks. If you are airborne reactive to corn, definitely call ahead and find out if one of these machines is in the office.
Ring Splints Can Help So Much
One of the things that can help you with hand pain whether you have a hand therapist or not is splints for your fingers. These come in two varieties, essentially- plastic and metal. To “prove” to myself that splints can help, I went ahead and ordered the plastic “oval 8” splints from Amazon.


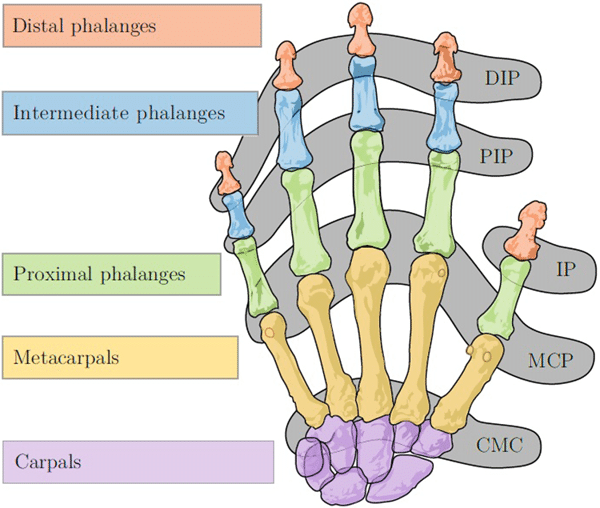
I got a LOT of function back instantly and a huge reduction in pain. I hadn’t even realized how much of my daily hand pain was from hyper-extension of my fingers. What was also unexpected was that my “knuckle” joints, aka my MCP joints, were stabilized by putting splints on my “middle” joints, also known as the PIP joints. So I didn’t just reduce pain in the joints I splinted – I reduced pain in my whole hand.
I got pretty “done” with my Oval 8’s pretty fast though because they don’t come in half-sizes, and my fingers definitely change size during the day, and they would start flying off my hands when swelling went down. Other people still prefer them to metal ring splints, though, and I’m told that some hand therapists can customize their sizing. Here’s an arthritis blog post comparing the two types.
Here’s what my hands look like wearing my silver ring splints along with my regular jewelry, plus a couple generic advertisement pictures for silver ring splints. The main reason I wear them is that they let me do basic tasks without screaming in pain, but they have the side effect of looking awesome.



You can purchase silver ring splints via orders from a hand therapist from SIRIS, at silverringsplint.com. Your hand therapist may go ahead and order and pay for them for you and bill you back for what isn’t covered, or they may ask you to pay ahead and submit later. Different CPT codes for the splints work better with different companies for better coverage, as each of these have a different max allowable amount, so if you get poor coverage or a denial you can always try resubmitting with a different code.
In either case, if you do run into issues with coverage, and appeals or resubmitting with a different code doesn’t work, it is totally possible to return ring splints to SIRIS as long as they are not damaged/are in sellable condition. I had a shockingly easy time getting mine covered, though. Your mileage may vary.
You can also purchase your own ring splints for cash from companies like Zebra Splints. If you decide to do this, I would consider the following:
- The way my hand therapist fitted my SIRIS splints was NOT the way I would have chosen to fit mine on my own, and she was absolutely more correct. So there is some value to having help with choosing and fitting your splints.
- Not all ring splints are created equal. Zebra Splints are quality, but the open-loop adjustable design of them may or may not work for your specific issues or habits. As for the other sellers, I’ve seen all kinds of poor practices and quality, from an inability to choose different sizing on each side of the joint on a non-adjustable splint, to just poor metal quality that people complain about getting rashes from.
Even if You “Only” Have Hypermobility Spectrum Disorder, You Still Need Medical Care for Your Symptoms
I’ve spent this entire post thus far explaining that hypermobility is NOT benign. If you have pain from your hypermobility, it needs treatment. If you don’t yet have pain from your hypermobility, that doesn’t mean you won’t. It is my opinion that you probably will eventually have pain from your hypermobility even if you don’t currently.
Many people with HSD, myself included, have some of the systemic effects of EDS even if they do not have enough of them currently to constitute a diagnosis. ALL of these effects are still medical problems that require treatment, and people with HSD need to be aware that they *could* develop more of these symptoms if they have one of them.
What Is Ehlers-Danlos Syndrome (EDS)?
Ehlers-Danlos Syndrome (EDS) refers to a group of heritable connective tissue disorders that cause abnormal connective tissue/collagen production. These disorders cause:
- All of the musculoskeletal, systemic, and chronic pain effects of HSD.
They also can (but may not always) cause the following:
- Soft/velvety skin which may or may not be fragile and hyper-extensible (stretchy)
- Organ prolapse/hernia
- Mitral valve prolapse/heart murmur
- problems with the meninge such as CSF leak
- Easy and often unexplained bruising
- Scarring and stretch marks out of proportion to the actual cause of the mark/scar
- Marfanoid Habitus
Some people with EDS have super stretchy skin, but not all. Many have a “forever young” look because their wacky collagen doesn’t sag and wrinkle as easily. Some start sagging weirdly at a very young age due to the collagen being weak. Some stay super young looking and then suddenly age “overnight.”
Depending on the type of EDS, the organ, vein, and central nervous system stuff may be better, worse, or mostly absent.
There are several subtypes of EDS that have a genetic mutation identified and you can test for these. All of these are of course rare. There is one, much more common, type of EDS called Hypermobile Type. Hypermobile Type has no known associated genetic subtype and can only be diagnosed via clinical observation.
Getting Diagnosed with Hypermobility Spectrum Disorder or Ehlers-Danlos Syndrome
The diagnostic criteria are quite clear, but it’s still hard to get doctors to make that diagnosis who aren’t familiar.
Not only that, but doctors who know just a little about EDS can be actually dangerous for us. I have seen reports in the patient community of doctors roughly pulling on their limbs and dislocating them “checking” for EDS, or from folks with VEDS, rough palpation of the abdomen actually causing organ perforation. Even if severe injuries like this don’t happen, an unfamiliar doctor may not recognize hypermobile joints even when looking at them, or may not realize they need to include historical hyperextension for adult patients who may have joint damage that limits the signs of hypermobility.
Your best bet for finding doctors who can diagnose Hypermobility and EDS is your patient community. Find someone else in your area who has been diagnosed, and see who diagnosed them.
Treatment for EDS and hypermobility is actually slightly easier than diagnosing it. Your biggest resource for treatment is going to be the patient community and your own learning. Find out who in your area is helping folks with similar issues, and self-educate so that you understand what kind of care you need.
Resources for Learning about and Managing EDS and Hypermobility
The following resources are invaluable for understanding your own conditions, and can also be used to help educate any providers you have that are willing to listen and learn alongside you.
- Disjointed: Navigating the Diagnosis and Management of hypermobile Ehlers-Danlos Syndrome
- Living Life to the Fullest with Ehlers-Danlos Syndrome: Guide to Living a Better Quality of Life While Having EDS by Kevin Muldowney, PT
- Understanding Hypermobile Ehlers-Danlos Syndrome and Hypermobility Spectrum Disorder by Claire Smith
- Hypermobility Without Tears: Moving Pain-Free with Hypermobility and EDS Paperback by Jeannie Di Bon
All of these books cover both hypermobility and EDS both. Even if you do have expert practitioners, I would still recommend reading one or more of these books for self-education.

Sweetie, I’m so sorry you have these conditions, however, I’m glad you’re diagnosed and found relief. God’s abundant blessings to you! Ambar in PR
My child also has this but we only found out after learning he has an autoinflammatory disease. Many with autoinflammatory diseases also have hEDS.
This is so incredibly amazing to see in print from other people! I too have hEDS and it used to be the party tricks and then it was subluxations my shoulders while eating or sleeping. And now that I’m in my 40’s the muscles are sooo tired of stretching so much and some joints are in constant flair which caused tendinitis in some areas and tendonitis in others.
And you have corn allergy issues as well!!! So glad I stumbled upon you in my searches for why I break out in hives and have stomach issues!!